Abstract
Background: Cytotoxic lesions of the corpus callosum (CLOCCs), particularly involving the splenium, are increasingly recognized on magnetic resonance imaging (MRI) in patients presenting with varied neurological and systemic symptoms. These lesions are typically transient, non-specific, and associated with a broad differential diagnosis, ranging from infections and metabolic disturbances to toxic and drug-related etiologies.
Case Presentation: A previously healthy 19-year-old female presented with fever and severe headache. Her only relevant past medical history was depression, managed with amitriptyline.
Imaging Findings and Laboratory Evaluation: On initial evaluation, physical examination and vital signs were normal, and an unenhanced head CT scan showed no acute abnormalities. Over the next 48 hours, the patient experienced clinical deterioration characterized by confusion, neck stiffness, and hypertension. Repeat physical examination noted mild disorientation, but no focal neurological deficits. Laboratory workup, including complete blood count, electrolytes, and renal function, was unremarkable. Cerebrospinal fluid (CSF) analysis following lumbar puncture was normal, with no evidence of infection or inflammation. MRI of the brain demonstrated a focal lesion in the splenium of the corpus callosum, hyperintense on T2-weighted and diffusion-weighted imaging (DWI), with corresponding low signal on the apparent diffusion coefficient (ADC) map, consistent with restricted diffusion. No enhancement was observed post-contrast.
Diagnosis and Management: Based on the characteristic imaging findings, a diagnosis of CLOCC was made. The patient was managed conservatively without steroids or immunoglobulin therapy. Her symptoms resolved within 24 hours. A follow-up MRI five days later revealed near-complete resolution of the lesion.
Discussion: CLOCCs have varied etiologies, including viral infections, metabolic derangements, seizures, and drug toxicity. In this case, other potential causes were ruled out through clinical evaluation and diagnostic testing, leaving amitriptyline toxicity as the most plausible etiology. The pathophysiology is believed to involve an inflammatory cascade leading to glutamate accumulation and subsequent cytotoxic edema. The splenium is particularly vulnerable due to its high density of glutamate receptors and oligodendrocytes. The imaging hallmark of CLOCC is a reversible, non-enhancing splenial lesion with restricted diffusion, often resolving within days. Recognition of these findings is critical to avoid unnecessary interventions. Treatment is supportive and tailored to the underlying cause. In cases of tricyclic antidepressant overdose, sodium bicarbonate remains the treatment of choice, though it was not required in this instance.
Conclusion: CLOCCs are reversible entities with distinctive imaging findings. They should be considered in young patients presenting with encephalopathic symptoms, particularly when infectious and metabolic causes are excluded. Drug toxicity, including from common antidepressants like amitriptyline, must be part of the differential. Early MRI can aid in diagnosis, guide appropriate management, and prevent overtreatment. This case highlights the importance of correlating clinical findings with imaging to arrive at a timely and accurate diagnosis.
CASE PRESENTATION
Presenting Illness
A 19-year-old female presented to the emergency department with fever and severe headache. The patient was previously healthy, except for a past medical history of depression, for which the patient is currently being treated with amitriptyline 75mg PO. The patient denied any use of tobacco, alcohol, or recreational drugs.
Physical Exam and Initial Workup
Vital signs were within normal range, including heart rate, respiratory rate, temperature, and blood pressure. Physical examination revealed a patient who was stable and was in no obvious distress.
Unenhanced Computed Tomography (CT) of the brain was performed, which was normal, with no acute cortical infarction or intracranial hemorrhage (Figure 1). The patient was admitted for further evaluation.
Figure 1: Normal unenhanced CT head, with no acute cortical infarction or intracranial hemorrhage
Clinical Course and Prognosis
During the initial 2 days of admission, the patient was clinically stable and under close observation. She was monitored supportively, until she experienced an acute clinical deterioration approximately 48 hours after admission. This was characterized by symptoms of fever, headache, neck stiffness and hypertension.
On repeat physical examination, the patient was slightly confused to time and place. The patient looked well otherwise. There was no motor weakness or sensory symptoms. Reflexes were normal.
Laboratory evaluation revealed normal complete blood count (CBC) and electrolytes. Renal function was also normal.
Given the symptoms of fever and neck stiffness, lumbar puncture was performed to obtain a cerebrospinal fluid (CSF) sample to rule out meningitis. On CSF analysis, there was no leukocytosis or abnormal cells. Microbiology was negative. All viral serology was negative.
Lumbar puncture, for direct cellular analysis of CSF, is the gold standard to assess for infection. While an MRI and/or a neurology consultation may be appropriate, they are not the most immediate steps. A toxicology screen could also be considered; however, the presence of fever makes an infectious cause more likely than a drug overdose.
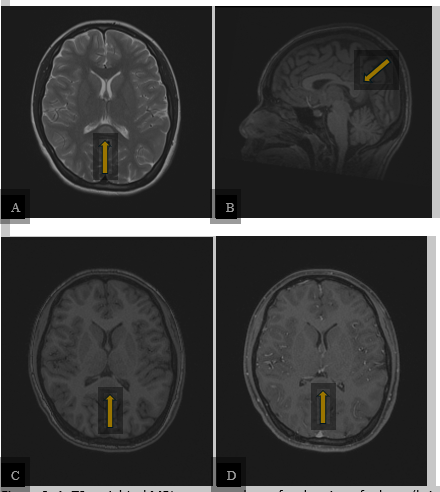
Magnetic Resonance Imaging (MRI) of the brain was performed and demonstrated a focal region of edema (bright T2 signal) within the splenium of the corpus callosum in the midline. This lesion was dark on T1 and showed no enhancement following intravenous contrast administration (Figure 2).
Figure 2: A. T2-weighted MRI sequence shows focal region of edema (bright signal) within the splenium of the corpus callosum in the midline (arrow). B. and C. This lesion was dark on T1-weighted sequence (arrows). D. The lesion showed no enhancement following intravenous contrast administration on the T1 post-contrast sequence (arrow). The rest of the brain was normal.
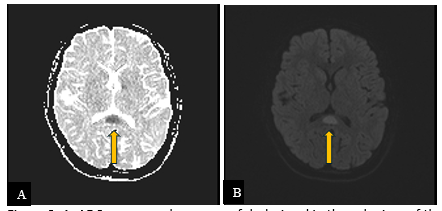
Diffusion-weighted imaging revealed bright signal with corresponding dark signal on ADC map, consistent with restricted diffusion (Figure 3). The rest of the brain was normal.
Figure 3: A. ADC map reveals an area of dark signal in the splenium of the corpus callosum (arrow). B. On diffusion-weighted imaging (DWI), there is corresponding bright signal (arrow). Imaging features are consistent with restricted diffusion.
A diagnosis of cytotoxic lesion of the corpus callosum (CLOCC) was made based on the characteristic imaging appearance.
The patient was managed conservatively, and her symptoms resolved within 24 hours without the need for aggressive intervention. A follow-up MRI performed 5 days later showed improvement with near complete resolution of the CLOCC (arrows) seen on the previous examination. There was no acute infarction (Figure 4).
Figure 4: A. T2-weigthed sequence shows near complete resolution of the focal region of edema (bright signal) within the splenium of the corpus callosum (arrow). B. and C. ADC map and DWI also show near complete resolution of restricted diffusion (bright signal) in the splenium (arrows) seen on the previous examination.
DISCUSSION
Cytotoxic lesion of the corpus callosum is a common magnetic resonance imaging finding [1], and it has various etiologies. Its prevalence is unknown, due to its variability in presentation [2]. Some patients are asymptomatic and do not necessitate neuroimaging. Symptoms are usually related to the etiology of the cytotoxic lesion of the corpus callosum more than the neuroanatomical territory itself [1]. Typical symptoms usually include fever, headache, confusion, and altered mental status [3].
Etiologies of CLOCC in this case could have been drug toxicity (antidepressants, antiepileptic, antipsychotics, or pesticide ingestion), seizures, metabolic disturbance (electrolyte imbalance, hemolytic-uremic syndrome, hypoglycemia, osmotic demyelination, or Wernicke's encephalopathy), or viral infection (influenza measles, herpes, mumps, adenovirus, rotavirus, SARS-CoV-2). Other causes include bacterial infections, malignancy, chemotherapy and subarachnoid hemorrhage [4].
The imaging hallmark of CLOCC is a reversible, non-enhancing splenial lesion with restricted diffusion, often resolving within days. The differential diagnosis based on patient presentation includes multiple sclerosis, given the patient is a young female. However, multiple sclerosis is unlikely given the lack of dissemination in time and space on MRI and the overall clinical picture. There was only one lesion as well, which makes this unlikely. Complex migraine is unlikely due to the absence of a migraine history and focal neurological deficits. Meningitis can be ruled out due to a normal lumbar puncture with no leukocytosis and negative microbiology.
The typical workup includes complete blood count and electrolytes to rule out a metabolic disturbance, a lumbar puncture, and neuroimaging if clinically indicated. In this case, an initial CT of the brain was ordered to rule out any causes of increased intracranial pressure. Two days later, the patient had neck stiffness, so a lumbar puncture was performed to rule out meningitis.
The pathophysiology of CLOCC is an initial trigger that causes macrophages to release inflammatory cytokines. All of this leads to a large buildup of glutamate outside cells, which then results in water entering astrocytes and neurons. This causes cytotoxic edema. The splenium of the corpus callosum is particularly affected because it contains many oligodendrocytes with a high number of glutamate-sensitive receptors [4].
In terms of treatment, some studies suggest the use of methylprednisolone and intravenous immunoglobulin to stop the cytokine storm [5]. However, no clinical benefit has been demonstrated. The typical treatment depends on the etiology of the CLOCC. For example, in patients with subarachnoid hemorrhage, treatment includes clipping or endovascular coil embolization [6].
A drug overdose with amitriptyline was implicated due to the patient’s history of depression. Other potential causes, such as infectious or metabolic etiologies, had been ruled out. Amitriptyline was the only plausible agent responsible for the toxicity, as the patient did not take any other medications and did not use any substances. The patient was referred to psychiatry for management.
Sodium bicarbonate is the standard of care for tricyclic antidepressant toxicity [7]. It improves cardiac conduction and hypotension.
Once the patient is medically stable, a psychiatry consultation is essential for optimizing treatment and assessing suicide risk. High-flow nasal cannula could have been appropriate in the context of respiratory compromise secondary to a viral or bacterial infection. Fluid therapy may play a role in dilution and clearance, but it is mainly used in the context of acute resuscitation (e.g., sepsis, hemorrhage) and for maintaining homeostasis. Finally, activated charcoal is used in cases of poisoning and is most effective when administered within a short window after toxin ingestion, particularly when no specific antidote exists.
Prognosis is dependent on the etiology of the disease. Typically, with appropriate treatment, there is both clinical and radiologic resolution of disease.
CONCLUSION
Cytotoxic lesions of the corpus callosum are reversible entities with distinctive imaging findings. They should be considered in young patients presenting with encephalopathic symptoms, particularly when infectious and metabolic causes are excluded. Drug toxicity, including from common antidepressants like amitriptyline, must be part of the differential. Early MRI can aid in diagnosis, guide appropriate management, and prevent overtreatment. This case highlights the importance of correlating clinical findings with imaging to arrive at a timely and accurate diagnosis.
Future directions could include standardized MRI follow-up and close correlation with biomarkers in early identification of etiology of Cytotoxic lesions of the corpus callosum.
Disclosure
Figures are first author’s own.
Queen’s University Health Sciences ethics approval received:
TRAQ #: 6043874
Patient consent is considered a component of and not specifically required for the Queen’s University Health Sciences ethics approval for case reports.
References
-
Moors S, Nakhostin D, Ilchenko D, Kulcsar Z, Starkey J, Winklhofer S, Ineichen BV (2023). Cytotoxic lesions of the corpus callosum: a systematic review. Eur Radiol. 2024 Jul;34(7):4628-4637. doi: 10.1007/s00330-023-10524-3. Epub. PMID: 38147170; PMCID: PMC11213749.
View
at Publisher
View
at Google Scholar
-
Soares M, Rosa S, Bettencourt S, Ferreira R, Sardinha M, Dias M, Cunha B (2024). Cytotoxic lesions of the corpus callosum due to FOLFIRINOX chemotherapy, Brain Disorders, Volume 15, 100157, ISSN 2666-4593
View
at Publisher
View
at Google Scholar
-
Procaccini L, Mincuzzi E, Bernardini A, Franchi P, Voicu IP, Caulo M (2022).
View
at Publisher
View
at Google Scholar
-
Gaillard F, Sharma R, Campos A, et al (2025). Cytotoxic lesions of the corpus callosum (CLOCCs). Reference article, Radiopaedia.org
View
at Publisher
View
at Google Scholar
-
Takanashi J, Shiihara T, Hasegawa T, Takayanagi M, Hara M, Okumura A, Mizuguchi M (2014). Clinically mild encephalitis with a reversible splenial lesion (MERS) after mumps vaccination. J Neurol Sci. 2015 Feb 15;349(1-2):226-8. doi: 10.1016/j.jns.2014.12.019. Epub. PMID: 25542078.
View
at Publisher
View
at Google Scholar
-
Toi H, Yagi K, Matsubara S, Hara K, Uno M (2021). Clinical Features of Cytotoxic Lesions of the Corpus Callosum Associated with Aneurysmal Subarachnoid Hemorrhage. AJNR Am J Neuroradiol. 2021 Jun;42(6):1046-1051. doi: 10.3174/ajnr.A7055. Epub. PMID: 33664118; PMCID: PMC8191652.
View
at Publisher
View
at Google Scholar
-
Odigwe CC, Tariq M, Kotecha T, Mustafa U, Senussi N, Ikwu I, Bhattarcharya A, Ngene JI, Ojiako K, Iroegbu N (2016). Tricyclic antidepressant overdose treated with adjunctive lipid rescue and plasmapheresis. Proc (Bayl Univ Med Cent).;29(3):284-7.
View
at Publisher
View
at Google Scholar


 :
© 2025 Omar Islam. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2025 Omar Islam. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.