Abstract
Introduction: Vesicouterine fistula (VUF) is a rare urogenital tract injury showing abnormal connection between the urinary bladder and the uterus,most commonly iatrogenic, following Caesarean Section(CS).
Case presentation: We report the case of a 31-year-old female (Gravida 4, Para 4, 2 CS) presenting with cyclic hematuria (menouria), malodorous vaginal discharge and dyspareunia. Physical examination revealed watery discharge from the cervix. Computed tomography (CT) cystography confirmed a fistulous communication between the posterosuperior bladder wall and anterior uterine wall.
Conclusion: The presence of menouria in multiparous women with history of CS is pathognomonic for Youssef’s Syndrome. CT cystography is a valuable diagnostic modality to confirmthe condition. Surgicalrepair remains the definitive treatment of choice.
INTRODUCTION
Vesicouterine fistula (VUF) is a rare entity showing abnormal connection between the urinary bladderand the uterus. It accounts for approximately 1%-4% of urogenital fistulas (Tarhanet al., 2019). It was first describedby Abdel Fattah Youssef in 1957, who identified the triad of cyclic hematuria (menouria), amenorrhea, and urinary continence, collectively known as “Youssef’s Syndrome” (Youssef, 1957).
Unlike Vesicovaginal fistula (VVF), typically presenting with continuous per-vaginal urineleakage, VUF symptoms are subtle and have a cyclic nature, resulting in delayed diagnosis.
Historically, the main aetiology of VUF was obstetric trauma (prolonged labour), which shifted over the past century to iatrogenic causes, specifically lower segment caesarean section (LSCS), now responsible for most of the cases (Bonavina et al., 2023). This case report discusses a multiparous patient with history of 2 CS, presentingwith the classic triad of Youssef Syndrome and diagnosed with Computed Tomography (CT) cystography.
CASE PRESENTATION
Patient Profile
A 31-year-old female, Para 4, Gravida 4, with historyof CS, presented to the gynaecology outpatient clinic.
History of Present Illness
The patient complained of a burning sensation during urination (dysuria) and a distinct, unpleasant odour to the urine. Her primary concern was cyclic hematuria (menouria), characterized by blood in the urine appearing specifically during menstruation, accompanied by discoloration. Following the onset of urinary symptoms, the patient noticed a vaginal discharge that was initially watery but progressed to become coloured and malodorous. She also reported significant dyspareunia.
Clinical Examination
Gynaecological Examination
Revealed normal external genitalia. On speculum examination, a pooling of watery fluidwas observed in the vaginal vault. Inspection of the cervix showed fluid propagation from thecervical os, raising clinicalsuspicion of an abnormal communication between the urinary and genital tracts.
Radiological investigation
A CT cystography was performed
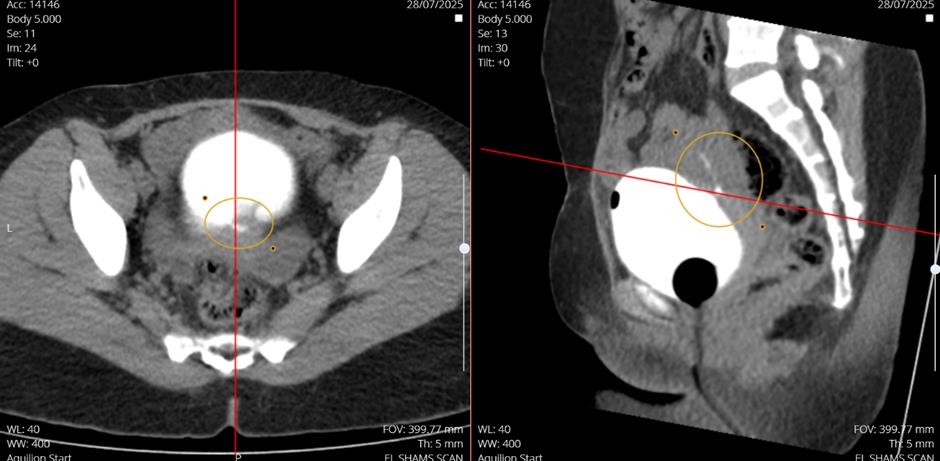
Findings: the imaging revealed a narrow fistulous connection between the posterior-superior surface of the urinary bladder and the overlying anterior uterine wall. Hyperattenuating water soluble contrast material was visualized extending from the bladder lumen to the uterine cavity (annotated axial and sagittal images).
- Incidental Finding: A left adnexal cyst measuring 47x28x44mm was identified.
- Diagnosis: Vesicouterine Fistula (Youssef’s syndrome).
Figure 01: Posterior-Superior surface of the urinary bladderand the overlying anterior uterine wall
DISCUSSION
Aetiology and Risk Factors
The incidence of VUF has increased in parallel with the rising rates of CS globally. The primary mechanism of injury involves the accidental inclusion of the posterior bladder wall into the uterineclosure suture during LSCS, or inadequate downward dissection of the bladderduring the procedure (Porcaro et al., 2002). Given this patient’s obstetric history, it is most likely that the previous CS contributed to the formation of the fistula.
Pathophysiology of Symptoms
The clinicalpresentation of VUF is unique
- Menouria: thishallmark symptom occursbecause of a pressure gradient. During menstruation, the intrauterine pressure increases due to uterine contractions, exceeding the intravesical pressure. This forces menstrual blood through the fistula into the bladder, resulting in cyclic hematuria (Di Marco et al., 2006).
- Urinary Continence versus incontinence: in “classic” Youssef’s Syndrome, patients remain continent because the fistula is located above the uterine isthmus, which acts as a competent sphincter preventing urine flow into the vagina. However, this patient presented with vaginal discharge, suggesting a “Type II” or mixed presentation where the fistulous track allows bidirectional flow-menstrual blood into the bladder and urine into the uterus/ vagina (Bonavina et al., 2023).
- Dysuria and Malodour: The burning sensation and smell reported by the patient are likely secondary to chronic cystitis by the introduction of menstrual debris and vaginal bacteria into the sterile bladder environment.
Diagnostic Imaging
While cystoscopy and hysterosalpingography have been used historically, CT cystography is currently considered the most effective imaging modality. As demonstrated in this case, CT cystography provides excellent anatomical detail, clearlydefining the size and locationof the tract and its relationship to adjacent structures (Kaur et al., 2018). It is superior to standard cystoscopy, which may fail to visualize small fistulous openings located in the bladder dome or posterior wall due to folding of the mucosa.
Management Strategies
Management of VUF depends on the time of diagnosis relative to the inciting surgery and the severity of symptoms.
Conservative Management: Spontaneous closure is possible in approximately 5% of cases, typically if diagnosed very early (within weeks of surgery). This involves continuous bladder drainage via a Foley catheter for 4 to 8 weeks to keep the bladder decompressed (Machado et al., 2019).
- Hormonal Therapy: induction of amenorrhea using oral contraceptives or Luteinizing Hormone-Releasing Hormone (LHRH)analogues can facilitate spontaneous closure by preventing the cyclic flow of menstrual blood through the tract (Tarhan et al., 2019).
- Surgical Repair: For patients with established, chronic fistulas (like the presented case) or failed conservative management, surgical repair is the gold standard. Techniques include:
- Open repair(Laparotomy): Separation of the bladder and uterus, excision of the fistulous tract, and interposition of an omental flap to preventrecurrence.
- Minimally Invasive Surgery: Laparoscopic and robotic-assisted repairs are increasingly preferred due to reduced morbidity and faster recovery times. The success rate for surgical repair approaches 100% in experienced hands (Abdel-Karim et al., 2016).
In this case, given the patient’s symptomatic burden (dysuria, menouria, and malodorous discharge), surgical intervention is recommended. The incidental left adnexal cyst should be evaluated further but does not alter the management plan for the fistula.
CONCLUSION
Vesicouterine Fistula should be strongly suspected in any woman with history of Caesarean section presenting with cyclic hematuria. This case validates the utility of CT cystography in confirming the diagnosis. While conservative management is an option for early cases, surgical repair remains the definitive treatment for symptomatic, chronic fistulas to restore quality of life and prevent recurrent urinary tract infections.
References
-
Bonavina, G., Busnelli, A., Acerboni, S., Martini, A., Candiani, M., & Bulfoni, A. (2023). Surgical repair of post-caesarean Vesicouterine fistula: A systemic review and a plea for prevention. International Journal of Gynecology & Obstetrics.
View
at Publisher
View
at Google Scholar
-
DiMarco, C. S., DiMarco, D. S., Klingele, C. J., & Gebhart, J. B. (2006). Vesicouterine fistula: a review of eight cases. International urogynecology journal and pelvic floor dysfunction, 17(4), 395–399.
View
at Publisher
View
at Google Scholar
-
Machado Junior, R. A., Machado Junior, L. C., & Lourenço e Lourenço, L. (2018). Vesicouterine fistula (Youssef syndrome): Case report and literature review [Fístula vesico-uterina (síndrome de Youssef): descrição de caso e revisão da literatura]. Revista Brasileira de Ginecologia e Obstetrícia, 40(9), 563–569.
View
at Publisher
View
at Google Scholar
-
Porcaro, A. B., Zicari, S., Zecchini Antoniolli, S., Pianon, R., Monaco, C., Migliorini, F., & Comunale, L. (2002). Vesicouterine fistula following caesarean section: Report of a case, review of the literature and proposed classification. European Urology, 41(2), 188-193.
View
at Publisher
View
at Google Scholar
-
Tarhan, F., Erbay, E., Penbegül, N., & Kuyumcuoğlu, U. (2007). Minimal invasive treatment of vesicouterine fistula: a case report. International urology and nephrology, 39(3), 791–793.
View
at Publisher
View
at Google Scholar
-
YOUSSEF A. F. (1957). Menouria following lower segment cesarean section; a syndrome. American journal of obstetrics and gynecology, 73(4), 759–767.
View
at Publisher
View
at Google Scholar


 :
© 2026 Mohammed Faez Baobaid. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
:
© 2026 Mohammed Faez Baobaid. This open-access article is distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.